| Curves, Bends, and Peyronie's Disease |
| ANDROLOGY : The Science of Dysfunctions of the Male Reproductive System |

Krishnamurti penile dermal flap operation for Peyronie's disease
 | |
| Sex is Not a Four-Letter Word | |
| Publisher: Rupa & Co., India | |
| A sex edutainment book by Dr. Sudhakar Krishnamurti... |
|
| Check with a good bookstore near you! | |
| Buy Online at | |
| • | Rediff Books  |
| • | Google.com |
| • | Amazon.com |
| • | NDTV Fabmall |
| • | Linux Bazar |
| A G A S S I 'Ageing, Gender, Andrology, & Sexual (Sciences), Society of India'
|
|
 Though ejaculation often occurs normally and is an intensely pleasurable sensation for most men, it is an extremely complex phenomenon that is regulated by many different systems. Hence, things often can, and do go wrong. |
 Impotence often comes without warning and can strike even the most virile stud like a bolt of lightning. How much of a risk do you face ? |
 Sex is man's second strongest instinct. An instinct that is second only to the survival instinct. This means that if a man's life is not immediately imperilled, the next thing he will automatically think of is sex. from WHAT EVERY ADULT NEEDS TO KNOW ABOUT IMPOTENCE |
The vacuum device is an external, non-invasive treatment option for impotence.
This device is available for purchase through this site.
Please Contact Us
More Information on non-invasive treatment options. More Details
 Before the advent of andrology, it was both thought and taught that impotence was psychological in origin. Epoch-making andrologic research in the past decade has shattered this myth and today it is known that in 80-90% of such cases, there is a physical (organic) cause rather than a purely psychological (functional) one. from THE SCIENCE OF ANDROLOGY |
 We've all heard of the barren wife. But what of barren husbands ? Can male infertility be cured ? The wife visits her gynecologist...so who is the husband supposed to consult ? find out in THE MALE FACTOR IN INFERTILITY |
The disease is named after an eighteenth century French surgeon, Francois Gigot de La Peyronie and afflicts about 1 percent of the adult male population. A study of the cross section of the penis in the human male shows that the organ has many layers. Peyronie's disease affects the tunica albuginea layer of the penis. It is commonest between ages 40 and 70 though no age is exempt. Even boys in their teens with Peyronie's disease have been described. The exact cause of this disease is not known and many theories abound about the probable mechanism of occurrence of this condition.
Most patients will present one or more of the following complaints:
Pain accompanies the lump in approximately two-thirds of all patients but is often self-limiting and disappears after the disease has run its full course. The lump (or plaque or nodule) is generally about a centimeter in size and is usually located on the upper midline. Sometimes, it may be much larger in size and in diffuse or multiple form.
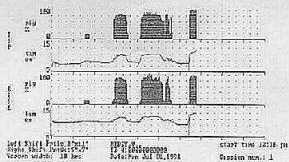
The lump may also be located at other areas on the penile shaft. The dorsal and ventral midlines are the common sites. The most important symptoms from the patient's and the clinician's standpoint are deformity on erection and impotence. Both these are common, and will require treatment. It is important for the examining clinician to be aware of the possibility of dealing with Peyronie's disease when he first sees the patient. Often, genital examination is conducted very perfunctorily and, in the absence of pain, a lump may be missed. It is also necessary to examine the penis in the erect position after the administration of a vasodilator drug like papaverine, phentolamine prostaglandin E1, or a combination of these. This allows accurate and objective measurement of the true extent of deformity and the degree of rigidity. Of course, all lumps on the penis are not secondary to Peyronie's disease. Additional investigations may include a 2 or 3 night computerised Rigiscan study for rigidity, a plain X-ray, and a flaccid penis ultrasound. Sometimes, it might be necessary to perform vascular studies (e.g. DICC, post-injection ultrasound), an MRI, etc.. The Rigiscan study gives a non-invasive and objective measurement of the patient's erection. Some people with Peyronie's disease may have impotence that is psychological in origin, rather than due to a true organic impairment. In such situations, the Rigiscan is invaluable for differentiating between the two. Shown below is a normal Rigiscan graph.
Besides, the Rigiscan also helps to detect disparity in penile base and tip rigidity which can occur because of the constricting effect of the lump. A plain soft tissue X-ray of the penis is useful in detecting the presence of calcific lesions. Approximately one-thirds of all patients with Peyronie's disease will develop calcific changes in the fibrous tissue of the lump. Calcification (deposition of calcium) generally denotes end-stage disease i.e. that the disease has run its full course and deformity and erection are not going to worsen further. This is useful in planning treatment. An ultrasound examination helps to demarcate the entire extent of the plaque (lump) - in all three dimensions. This is of great value if the Andrologist is contemplating operative intervention since a decision can be made about the type of operation suitable for employment in a given patient. The ultrasound examination can be further coupled with injections of vaso-active substances to study the arteries of the penis.
The aims of treatment are:
Several treatment modalities have been employed in the past to reduce pain and arrest the progression of the fibrotic process. These include several oral medications, X-ray therapy, topical applications, electrical therapy, ultrasonic treatment and locally injectable agents. None has so far proved conclusively superior to others, and benefits derived are probably sympathetic, placebo (psychological) or because of the self-limiting nature of the illness in some cases.
It must be remembered that, in some cases, Peyronie's disease runs quite a benign and self-limiting course. Such patients are fortunate and will require little or no therapeutic interference. In fact, needless administration (especially of intra-penile steroid injections, which are commonly used) can be damaging. After the disease has run its course it may even be possible for the patient, with his minimal penile deformity to rehabilitate himself quite well sexually. On the other end of the spectrum, of course, we have the much less fortunate patient, who not only has severe deformity (greater than 30 degrees) but also has severe impotence and just cannot perform sexually. Superimposed on these is always the element of depression. Such patients will require surgery especially if 12 to 18 months have elapsed since the first symptom appeared, and all other treatment forms have failed.
Many operations are available for the surgical treatment of this condition. The choice of operation in a given case will depend on the location of the lump, the extent of the lump and the degree of deformity caused, the presence or absence of superimposed organic impotence and the preferences of the operating Andrologist.
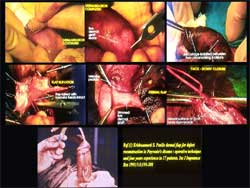
This is a drawback inherent in all free grafts because these are known to contract. Besides, foreign grafts (synthetic and animal) will also stimulate the formation of fibrous tissue and contraction. The only way to minimise these problems, i.e. to avoid contraction and impotence, is to use a FLAP (with its own blood supply) rather than a graft. The penile dermal graft described by Dr. Sudhakar Krishnamurti, the Chief Consultant of this site, is one such. Flaps have their own blood supply and hence are not prone to contract.
Step-wise Photographic Representation of the Penile Dermal Flap (Krishnamurti) Operation for Peyronie's Disease along with Original Reference (or) Download PDF (5658 KB)
Generally speaking, operations for Peyronie's disease should be performed with prudence and only by the experienced. Premature and inadequate surgery can be disastrous and can have a high recurrence/failure rate. Though the results of surgery are, by and large, satisfactory, the re-operation rate in patients operated upon improperly, is quite high. "Wait and watch : operate only when all else fails or disability is severe", seems a good maxim. Peyronie's disease is not uncommon and can sometimes be a crippling disease of the penis. Presenting usually as a lump in the midline shaft, it can cause deformity on erection and impotence. It especially affects the middle-aged and elderly. The exact cause of the condition is not known. The disease is sometimes self-limiting and disability is minimal. More severe deformity and impotence will require treatment, sometimes surgical. Surgery should be performed as a last resort and only by those especially experienced in dealing with this condition. Picture below shows the 'Surgical Treatment' Sub-Committee of the ISSM Standards Committee: Dr. Sudhakar Krishnamurti is seen at Bottom (Right)
Apart from Peyronie's Disease, there are other causes of penile curvature and deformity. Many of these are congenital (present from birth). Some are associated with conditions of the urethra. Some are not. In the latter situation, the penis appears absolutely normal in the flaccid (non-erect) state. Most patients have no impairment of rigidity and are capable of good erections. However, sometimes the deformity is severe enough to preclude peno-vaginal penetration and can also cause serious psychosexual disturbances. Both these situations will warrant surgical intervention. Surgery is simple, safe and gives very good results with complete straightening of the penis. Surgeries for Peyronie's Disease and penile curvatures are being regularly performed at Andromeda Andrology Center by Dr. Sudhakar Krishnamurti for the past sixteen years.
|
| |||||||||||||||||||||||||||||||
Home | News | Main Articles | Special Features | ||||||||||||||||||||||||||||||||